Assessment |
Biopsychology |
Comparative |
Cognitive |
Developmental |
Language |
Individual differences |
Personality |
Philosophy |
Social |
Methods |
Statistics |
Clinical |
Educational |
Industrial |
Professional items |
World psychology |
Clinical: Approaches · Group therapy · Techniques · Types of problem · Areas of specialism · Taxonomies · Therapeutic issues · Modes of delivery · Model translation project · Personal experiences ·

{kind=link}
| Alternative medical systems - edit |
|---|
| NCCAM classifications [4] |
|
1. Alternative Medical Systems |
| See also |
|
|
Chiropractic is a complementary and alternative health care profession which diagnoses and treats mechanical disorders of the spine and musculoskeletal system with the intention of affecting the nervous system and improving health.[1] It is based on the premise that a spinal joint misalignment, which chiropractors call a vertebral subluxation, can interfere with the nervous system and result in many different conditions of diminished health.[2] Treatments typically include spinal adjustments to correct the vertebral subluxation, though some may use other holistic interventions as well. In contrast, the term subluxation, as used in conventional medicine, is usually associated with specific conditions which are a direct consequence of injury to joints or associated nerves.
Chiropractic was founded in 1895 by DD Palmer. It is now licensed in every state in America and practiced in more than 100 countries.[3][4] Chiropractic's history includes conflicts within the profession and attacks from those outside the profession.
There are four main groups of chiropractors: "traditional straights", "objective straights", "mixers", and "reform". All groups, except reform treat patients using a subluxation-based system. Differences are based on the philosophy for adjusting, claims made about the effects of those adjustments, and various additional treatments provided along with the adjustment.
History[]
Chiropractic was founded in 1895 by Daniel David Palmer, based on his assertion that all health problems could be prevented or treated using adjustments of the spine (spinal adjustments), and sometimes other joints, to correct what he termed vertebral subluxations. He, and later his son B.J. Palmer, proposed that subluxations were misaligned vertebrae which caused nerve compression that interfered with the transmission of what he named Innate Intelligence. This interference interrupted the proper flow of Innate Intelligence from "above, down, inside, and out" to the organ to which it traveled. As a result, the human body would experience "dis-ease" or disharmony which would result in loss of health. He compared this process to stepping on a hose that slowed the flow of water to a garden: if you take your foot off the hose, the flow returns to normal and the garden will flourish.
Explanation[]
Manipulation of the spine is the main technique in today's chiropractic adjustment, or treatment. Though its use has been documented from the time of the ancient Egyptians,[5] spinal manipulation in an attempt to correct the theoretical vertebral subluxation is solely a chiropractic endeavor. Chiropractic's contribution to the field of manipulative therapies is the concept of applying a precise adjustment to a specific affected vertebra, as opposed to the generalized maneuvers of the early osteopaths. While some chiropractors adhere strictly to the use of only spinal manipulation in their adjustment, others include a broad range of methods directed at correcting the subluxation and/or just relieving musculoskeletal pain.
Some chiropractors specialize in treating specific musculoskeletal problems or sports injuries, or they may combine chiropractic with manipulation of the extremities, physiotherapy, nutrition, or exercises to increase spinal strength or improve overall health. Some also use other complementary and alternative methods as a part of a holistic treatment approach. However, chiropractors do not prescribe drugs; they believe this to be the province of conventional medicine, and that their role is to pursue drug-free alternative treatments. Depending on the country or state in which the Chiropractic school is located, some train in minor surgery. When indicated, the doctor of chiropractic consults with, co-manages, or refers to other health care providers.[6]
Theories[]
While the "pinched garden hose theory" has mostly been abandoned, it is still used in a modified form by some chiropractors to explain vertebral subluxation. However, the concept of the subluxation, which has marginal evidence, remains integral to typical chiropractic practice. In 2003, 90% of chiropractors believed the vertebral subluxation complex played a significant role in all or most diseases.[7]
There is evidence that spinal manipulation is effective for the treatment of acute low back pain, tension headaches and some musculoskeletal issues, but not all studies support this conclusion.[8][9] There are no objective controlled trials with definitive conclusions for or against chiropractic claims concerning other health benefits.[10]
Origins of Chiropractic and the concept of subluxation[]
{kind=link}
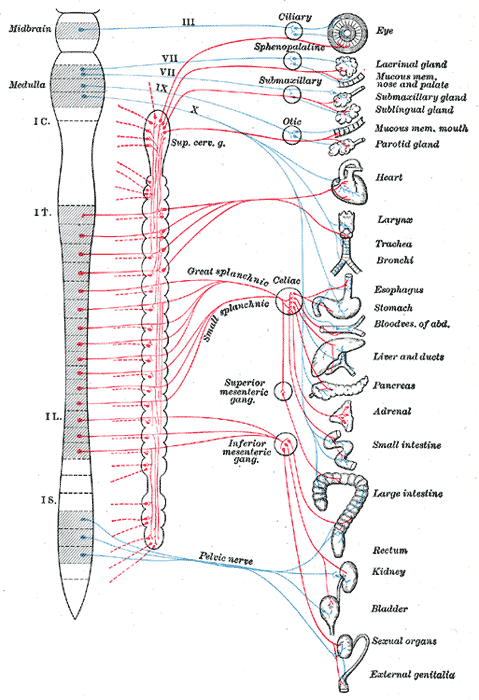
Autonomic Nervous System
Blue = parasympathetic
Red = sympathetic
- Main article: Vertebral subluxation
DD Palmer, using a vitalistic approach, imbued the term subluxation with a metaphysical and philosophical meaning. He held that a malposition of spinal bones, which protect the spinal cord and nerve roots, interfered with the transmission of nerve impulses. Because half of the nervous system is sensory and the other half motor (control), he postulated that living things had an Innate intelligence, a kind of "spiritual energy" or life force that received the sensory information from the various parts of the body and made a decision as to what the motor nerves should convey. DD Palmer claimed that subluxations interfered with this innate intelligence, and that by fixing them, all diseases could be treated.[11] He qualified this by noting that knowledge of Innate Intelligence was not essential to the competent practice of chiropractic.[12] The idea that all diseases were the result of a subluxation was in line with the common thinking of the day; that there was one cause for disease. The vitalistic concepts implied an intelligent governing entity that was readily perceived as spiritual constructs by many both inside and outside the profession. Chiropractors used these metaphorical concepts to rationalize their thinking about the body’s self-healing capacity.[13] In 1998, Lon Morgan DC, a reform chiropractor, wrote that: "Innate Intelligence clearly has its origins in borrowed mystical and occult practices of a bygone era. It remains untestable and unverifiable and has an unacceptably high penalty/benefit ratio for the chiropractic profession. The chiropractic concept of Innate Intelligence is an anachronistic holdover from a time when insufficient scientific understanding existed to explain human physiological processes. It is clearly religious in nature and must be considered harmful to normal scientific activity."[14]
Meridel I. Gatterman DC, educator and writer observed:
- "The word subluxation has been ... embodied with a multitude of meaning by chiropractors during the past one hundred years. To some it has become the holy word; to others, an albatross to be discarded ... to add to the confusion, more than 100 synonyms for subluxation have been used. Why then do we persist in using the term when it has become so overburdened with clinical, political, and philosophical ... significance ... that the concept that once helped to hold a young profession together now divides it and keeps it quarrelling over basic semantics? The obvious answer is: The concept of subluxation is central to chiropractic."[15]
Debate about the need to remove the concept of subluxation from the chiropractic paradigm has been ongoing since the mid 1960s. While straights hold firmly to the term and its vitalistic construct, reformers suggest that the mechanistic model will allow chiropractic to better integrate into mainstream medicine without making claims inherent in the term. Anthony Rosner PhD, director of education and research at the Foundation for Chiropractic Education and Research (FCER) considered subluxation and the concept of Occam's razor. He suggests "there is no obvious reason to discard the concept of subluxation, while at the same time maintaining that it is not a rigid entity, but rather an important model and concept; a work in progress that undoubtedly will undergo extensive modification as our concepts of light or psychoanalysis have evolved over half a century."[16]
Despite the term's vitalistic roots, chiropractic today may still use the term Innate Intelligence; however, it has taken on a less metaphysical meaning. Innate Intelligence today is used to describe the self-healing power of the body. Thus, a modern chiropractic view is that by removing the restrictions caused by subluxation, the chiropractor is improving the body's own potential for self-healing. [17]
Chiropractic’s approach to healthcare[]
According to Robert Mootz D.C. and Reed Phillips D.C., Ph.D., although chiropractic has much in common with other health professions, its philosophical approach distinguishes it from modern medicine. Chiropractic philosophy involves what has been described as a "contextual, naturopathic approach" to health care.[18] The traditional, "allopathic" or "medical" model considers disease as generally the result of some external influence, such as a toxin, a parasite, an allergen, or an infectious agent: the solution is to counter the perceived environmental factor (e.g., using an antibiotic for a bacterial infection). By contrast, the naturopathic approach considers that lowered "host resistance" is necessary for disease to occur, so the appropriate solution is to direct treatment to strengthen the host, regardless of the environment. In contemporary clinical practice, one can find elements of both naturopathic and allopathic philosophy among all types of providers.[13] The degree to which a practitioner emphasizes different tenets of these philosophies is one factor that determines the manner in which they practice.
- Chiropractic Perspectives That Reflect a Holistic Approach to Patient Care
- noninvasive, emphasizes patient's inherent recuperative abilities
- recognizes dynamics between lifestyle, environment, and health
- emphasizes understanding the cause of illness in an effort to eradicate, rather than palliate, associated symptoms
- recognizes the centrality of the nervous system and its intimate relationship with both the structural and regulatory capacities of the body
- appreciates the multifactorial nature of influences (structural, chemical, and psychological) on the nervous system
- balances the benefits against the risks of clinical interventions
- recognizes as imperative the need to monitor progress and effectiveness through appropriate diagnostic procedures
- prevents unnecessary barriers in the doctor-patient encounter
- emphasizes a patient-centered, hands-on approach intent on influencing function through structure
- strives toward early intervention, emphasizing timely diagnosis and treatment of functional, reversible conditions
- Source:AHCPR Chapter 2 Chiropractic Belief Systems, Robert D. Mootz DC; Reed B. Phillips DC, PhD
The Chiropractic approach to healthcare stresses the importance of prevention. Former president of National College of Chiropractic, Joseph Janse DC (1909-1985) explains:
- "Unless pathology is demonstrable under the microscope, as in the laboratory or by roentgenograms, to them [allopaths] it does not exist. For years the progressive minds in chiropractic have pointed out this deficiency. With emphasis they [chiropractors] have maintained the fact that prevention is so much more effective than attempts at a cure. They pioneered the all-important principle that effective eradication of disease is accomplished only when it is in its functional (beginning) phase rather than its organic (terminal) stage. It has been their contention that in general the doctor, the therapist and the clinician have failed to realize exactly what is meant by disease processes, and have been satisfied to consider damaged organs as disease, and to think in terms of sick organs and not in terms of sick people. In other words, we have failed to contrast disease with health, and to trace the gradual deteriorization along the downward path, believing almost that mild departures from the physiological normal were of little consequence, until they were replaced by pathological changes..."
Most patients who visit a chiropractor do so initially with a chief complaint related to musculoskeletal problems (especially low back and neck pain), although most chiropractors say they concern themselves with the overall health of the patient. According to a survey by the National Center for Complementary and Alternative Medicine, in 2002, chiropractic was the fourth (7.5%) most commonly used CAM therapy among adults in the USA.[19][20] The profession has evolved so that treatment consists of hundreds of different techniques.[21] The U.S. Department of Labor's Occupational Outlook Handbook said:
- Because chiropractors emphasize the importance of healthy lifestyles and do not prescribe drugs or perform surgery, chiropractic care is appealing to many health-conscious Americans. Chiropractic treatment of the back, neck, extremities, and joints has become more accepted as a result of research and changing attitudes about alternative, noninvasive health care practices.[22]
Most DCs are in private practice or work in small groups, employing chiropractic assistants as office staff and to perform therapeutic activities. They may also employ massage and physiotherapists as adjuncts to chiropractic care.
History[]
- Main article: Chiropractic history
{kind=link}
DD Palmer
DD Palmer gave the first chiropractic adjustment to a deaf janitor, Harvey Lillard, on September 18, 1895.

{kind=link}
Rev. Samuel Weed
Friend and Rev. Samuel Weed suggested combining the words cheiros and praktikos (meaning "done by hand") to describe Palmer's treatment method, creating the term "chiropractic." In 1896, DD added a school to his magnetic healing infirmary, and began to teach others his method. It would be become known as Palmer School of Chiropractic (PSC, now Palmer College of Chiropractic).
Medicine vs. chiropractic[]
In September 1899, a medical doctor in Davenport, IA, named Heinrich Matthey started a campaign against drugless healers in Iowa. DD Palmer, whose school had just graduated its 7th student, insisted that his techniques did not need the same courses or license as medical doctors, as his graduates did not prescribe drugs or evaluate blood or urine. However, in 1906, Palmer was convicted for practicing medicine without a license. He chose to turn over his interests in the PSC to his son, BJ and wife, Mabel.
BJ Palmer re-develops chiropractic[]

{kind=link}
BJ Palmer Developer of Chiropractic 1882-1961
BJ created the Universal Chiropractic Association (UCA) for the purpose of protecting its members by covering their legal expenses should they get arrested.[23] Its first case came in 1907, when Shegataro Morikubo DC of Wisconsin was charged with unlicensed practice of osteopathy. Morikubo was freed using the defense that chiropractic philosophy was different than osteopathic philosophy. The victory reshaped the development of the chiropractic profession, which then marketed itself as a science, an art and a philosophy, and BJ Palmer became the "Philosopher of Chiropractic".
Straight versus mixer[]
State laws to regulate and protect chiropractic practice were eventually introduced in all fifty states in the US, but it was a hard-fought struggle. Medical Examining Boards worked to keep all healthcare practices under their legal control, but an internal struggle among DC's on how to structure the laws significantly complicated the process. Initially, the UCA, led by BJ Palmer and armed with his philosophy, opposed state licensure altogether. Palmer feared that such regulation would lead to allopathic control of the profession.[24] The UCA eventually caved in, but BJ remained strong in the opinion that examining boards should be composed exclusively of chiropractors (not those who mixed chiropractic with other remedies). Mixers campaigned to increase education standards equivalent to medical schools while Palmer resisted any increase in standards.
The movement toward science[]
In 1975, the National Institutes of Health brought chiropractors, osteopaths, medical doctors and Ph.D. scientists together in a conference on spinal manipulation to develop strategies to study the effects of spinal manipulation. In 1978, the Journal of Manipulative & Physiological Therapeutics (JMPT) was launched, and in 1981 it was included in the National Library of Medicine's Index Medicus.[25] Joseph Keating dates the birth of chiropractic as a science to a 1983 commentary in the JMPT entitled "Notes from the (chiropractic college) underground" in which Kenneth F. DeBoer, then an instructor in basic science at Palmer College in Iowa, revealed the power of a scholarly journal (JMPT) to empower faculty at the chiropractic schools. DeBoer's opinion piece demonstrated the faculty's authority to challenge the status quo, to publicly address relevant, albeit sensitive, issues related to research, training and skepticism at chiropractic colleges, and to produce "cultural change" within the chiropractic schools so as to increase research and professional standards. It was a rallying call for chiropractic scientists and scholars.[25]
Wilk et al. vs the American Medical Association (AMA)[]
- Main article: Wilk v. American Medical Association
Until 1983, the AMA held that it was unethical for medical doctors to associate with an "unscientific practitioner", and labeled chiropractic "an unscientific cult". Principle 3 of the AMA Principles of Medical Ethics stated:
- "A physician should practice a method of healing founded on a scientific basis; and he should not voluntarily professionally associate with anyone who violates this principle."
Armed with Sore Throat's information about the methods of the Committee on Quackery, Chicago chiropractor, Chester A. Wilk initiated an antitrust suit against the AMA and other medical associations in 1976 - Wilk et al. vs AMA et al..[26] The landmark lawsuit ended in 1987 when the US District Court found the AMA guilty of conspiracy and restraint of trade; the Joint Council on Accreditation of Hospitals and the American College of Physicians were exonerated. The court recognized that the AMA had to show its concern for patients, but was not persuaded that this could not have been achieved in a manner less restrictive of competition, for instance by public education campaigns. The AMA lost its appeal to the Supreme Court, and had to allow its members to collaborate with DCs.[27]
Judge Susan Getzendanner, who presided over the Wilk case, said:
- "Evidence at the trial showed that the defendants took active steps, often covert, to undermine chiropractic educational institutions, conceal evidence of the usefulness of chiropractic care, undercut insurance programs for patients of chiropractors, subvert government inquiries into the efficacy of chiropractic, engage in a massive disinformation campaign to discredit and destabilize the chiropractic profession and engage in numerous other activities to maintain a medical physician monopoly over health care in this country."
She then said that chiropractors clearly wanted "a judicial pronouncement that chiropractic is a valid, efficacious, even scientific health care service". She said no "well designed, controlled, scientific study" had been done, and concluded "I decline to pronounce chiropractic valid or invalid on anecdotal evidence, even though "the anecdotal evidence in the record favors chiropractors".[27]
Scientific investigation of chiropractic[]
The Testable Principle The Untestable Metaphor Chiropractic Adjustment Universal Intelligence Restoration of structural integrity Innate Intelligence Improvement of Health Status Body Physiology Materialistic Vitalistic Operational definitions possible Origin of Holism in chiropractic lends itself to scientific inquiry cannot be proved or disproved Table 1. Two chiropractic system constructs. Source: Phillips RB, Mootz RD. Contemporary chiropractic philosophy. In Haldeman S (ed). Principles and Practice of Chiropractic, 2nd Ed. Norwalk, CT: Appleton & Lange, 1992. Chart reprinted from Keating J (1995), D.D. Palmer's Forgotten Theories of Chiropractic[5]
Chiropractic researchers Robert Mootz and Reed Phillips suggest that, in chiropractic's early years, influences from both straight and mixer concepts were incorporated into its construct. They conclude that chiropractic has both materialistic qualities that lend themselves to scientific investigation and vitalistic qualities that do not (Table 1).
With relatively little federal funding, academic research in chiropractic has only recently become established in the USA. In 1994 and 1995, half of all grant funding to chiropractic researchers was from the US Health Resources and Services Administration (7 grants totaling $2.3 million). The Foundation for Chiropractic Education and Research (11 grants, $881,000) and the Consortium for Chiropractic Research (4 grants, $519,000) accounted for most of the rest. By 1997, there were 14 peer-reviewed chiropractic journals in English that encouraged the publication of chiropractic research, including The Journal of Manipulative and Physiological Therapeutics (JMPT), Topics in Clinical Chiropractic, and the Journal of Chiropractic Humanities. However, of these, only JMPT is included in Index Medicus. Research into chiropractic, whether from Universities or chiropractic colleges, is however often published in many other scientific journals.[28]
While there is still debate about the effectiveness of chiropractic for the many conditions in which it is applied, chiropractic seems to be most effective for acute low back pain and tension headaches.[8] When testing the efficacy of health treatments, double blind studies are generally considered acceptable scientific rigor. These are designed so that neither the patient nor the doctor knows whether they are using the actual treatment or a placebo (or "sham") treatment. However, chiropractic treatment involves a manipulation; no "sham" procedure can be devised easily for this, and even if the patient is unaware whether the treatment is a real or sham procedure, the doctor cannot be unaware. Thus there may be "observer bias" - the tendency to see what you expect to see, and the potential for the patient to wish to report benefits to "please" the doctor. This problem is not confined to chiropractic - many medical treatments are not amenable to double-blind placebo-controlled trials, indeed this is true for all surgical procedures. It is also a problem in evaluating treatments; even when there are objective outcome measures, the placebo effect can be very substantial. Thus, DCs have historically relied mostly on their own clinical experience and the shared experience of their colleagues, as reported in case studies, to direct their treatment methods. In this, they are not different to the practice in much of conventional medicine.
Sociologist Leslie Biggs interviewed 600 Canadian DCs in 1997: while 86% felt that chiropractic methods needed to be validated, 74% did not believe that controlled clinical trials were the best way to evaluate chiropractic. Moreover, 68% believed that "most diseases are caused by spinal malalignment", although only 30% agreed that "subluxation was the cause of many diseases".[29]
Even when a valid mechanism of action is not determined, it is generally thought sufficient to present evidence showing benefit for the claims made. There is wide agreement that, where applicable, an evidence based medicine framework should be used to assess health outcomes, and that systematic reviews with strict protocols are important for objectively evaluating treatments. Where evidence from such reviews is lacking, this does not necessarily mean that the treatment is ineffective, only that the case for a benefit of treatment may not have been rigorously established.
A 2005 editorial in JMPT, "The Cochrane Collaboration: is it relevant for doctors of chiropractic?"[30] proposed that involvement in Cochrane collaboration would be a way for chiropractic to gain greater acceptance within medicine. The collaboration has 11,500 contributors from more than 90 countries organized in 50 review groups. For chiropractic, relevant review groups include the Back Group; the Bone, Joint, and Muscle Trauma Group; the Musculoskeletal Group; and the Neuromuscular Disease Group. The editorial states that, for example, "a chiropractor may provide conservative care supported by a Cochrane review to a patient with carpal tunnel syndrome. If the patient's symptoms become progressive, the doctor may consider referring the patient for surgery using a recent Cochrane review that examined new surgical techniques compared with traditional open surgery..."
The Cochrane Collaboration did not find enough evidence to support or refute the claim that manual therapy (including, but not limited to, chiropractic) is beneficial for asthma. Carpal tunnel syndrome trials have not shown benefit from diuretics, non-steroidal anti-inflammatory drugs, magnets, laser acupuncture, exercise or chiropractic and there is not enough evidence to show the effects of spinal manipulation (including, but not limited to, chiropractic) for painful menstrual periods. Bandolier found limited evidence that spinal manipulative therapy (including, but not limited to, chiropractic) might reduce the frequency and intensity of migraine attacks, but the evidence that spinal manipulation is better than amitriptyline, or adds to the effects of amitriptyline, is insubstantial for the treatment of migraine, although "spinal manipulative therapy might be worth trying for some patients with migraine or tension headaches."
According to Bandolier, a systematic review of a small, poor quality set of trials, provided no convincing evidence for long-term benefits of chiropractic interventions for acute or chronic low back pain, despite some positive overall findings [6] but there might be some short-term pain relief, especially in patients with acute pain.[31] However, the BMJ noted in a study on long-term low-back problems "...improvement in all patients at three years was about 29% more in those treated by chiropractors than in those treated by the hospitals. The beneficial effect of chiropractic on pain was particularly clear."[32] A 1994 study by the U.S. Agency for Health Care Policy and Research (AHCPR) and the U.S. Department of Health and Human Services endorses spinal manipulation for acute low back pain in adults in its Clinical Practice Guideline.
The first significant recognition of the appropriateness of spinal manipulation for low back pain was performed by the RAND Corporation. This meta-analysis concluded that some forms of spinal manipulation were successful in treating certain types of lower back pain. Some chiropractors claimed these results as proof of chiropractic hypotheses, but RAND's studies were about spinal manipulation, not chiropractic specifically, and dealt with appropriateness, which is a measure of net benefit and harms; the efficacy of chiropractic and other treatments were not explicitly compared. In 1993, Dr Shekelle rebuked some DCs for their exaggerated claims: ...we have become aware of numerous instances where our results have been seriously misrepresented by chiropractors writing for their local paper or writing letters to the editor....[33]
There is conflict in the results of chiropractic research. For instance, many DCs claim to treat infantile colic. According to a 1999 survey, 46% of chiropractors in Ontario treated children for colic. [34] In 1999 a Danish randomized controlled clinical trial with a blinded observer suggested that there is evidence that spinal manipulation might help infantile colic.[35] However, in 2001, a Norwegian blinded study concluded that chiropractic spinal manipulation was no more effective than placebo for treating infantile colic.[36]
In 1997, historian Joseph Keating Jr described chiropractic as a "science, antiscience and pseudoscience", and said "Although available scientific data support chiropractic's principle intervention method (the manipulation of patients with lower back pain), the doubting, skeptical attitudes of science do not predominate in chiropractic education or among practitioners". He argued that chiropractic's culture has nurtured antiscientific attitudes and activities, and that "a combination of uncritical rationalism and uncritical empiricism has been bolstered by the proliferation of pseudoscience journals of chiropractic wherein poor quality research and exuberant over-interpretation of results masquerade as science and provide false confidence about the value of various chiropractic techniques". However, in 1998, after reviewing the articles published in the JMPT from 1989-1996, he concluded,
- "substantial increases in scholarly activities within the chiropractic profession are suggested by the growth in scholarly products published in the discipline's most distinguished periodical (JMPT). Increases in controlled outcome studies, collaboration among chiropractic institutions, contributions from nonchiropractors, contributions from nonchiropractic institutions and funding for research suggest a degree of professional maturation and growing interest in the content of the discipline."[37]
The Manga Report[]
The Manga Report was an outcomes-study funded by the Ontario Ministry of Health and conducted by three health economists led by Professor Pran Manga. The Report supported the scientific validity, safety, efficacy, and cost-effectiveness of chiropractic for low-back pain, and found that chiropractic care had higher patient satisfaction levels than conventional alternatives. The report states that "The literature clearly and consistently shows that the major savings from chiropractic management come from fewer and lower costs of auxiliary services, fewer hospitalizations, and a highly significant reduction in chronic problems, as well as in levels and duration of disability."[38]
Workers' Compensation studies[]
In 1998, a study of 10,652 Florida workers' compensation cases was conducted by Steve Wolk. He concluded that "a claimant with a back-related injury, when initially treated by a chiropractor versus a medical doctor, is less likely to become temporarily disabled, or if disabled, remains disabled for a shorter period of time; and claimants treated by medical doctors were hospitalized at a much higher rate than claimants treated by chiropractors."[39] Similarly, a 1991 study of Oregon Workers' Compensation Claims examined 201 randomly selected workers' compensation cases that involved disabling low-back injuries: when individuals with similar injuries were compared, those who visited DCs generally missed fewer days of work than those who visited MDs.[40]
A 1989 study analyzed data on Iowa state records from individuals who filed claims for back or neck injuries. The study compared benefits and the cost of care from MDs, DCs and DOs, focusing on individuals who had missed days of work and who had received compensation for their injuries. Individuals who visited DCs missed on average 2.3 fewer days than those who visited MDs, and 3.8 fewer days than those who saw DOs, and accordingly, less money was dispersed as employment compensation on average for individuals who visited DCs.[41]
In 1989, a survey by Cherkin et al. concluded that patients receiving care from health maintenance organizations in the state of Washington were three times as likely to report satisfaction with care from DCs as they were with care from other physicians. The patients were also more likely to believe that their chiropractor was concerned about them.[42]
American Medical Association (AMA)[]
In 1997, the following statement was adopted as policy of the AMA after a report on a number of alternative therapies:[7]
Specifically about chiropractic it said,
- "Manipulation has been shown to have a reasonably good degree of efficacy in ameliorating back pain, headache, and similar musculoskeletal complaints."
In 1992, the AMA issued this statement:
- "It is ethical for a physician to associate professionally with chiropractors provided that the physician believes that such association is in the best interests of his or her patient. A physician may refer a patient for diagnostic or therapeutic services to a chiropractor permitted by law to furnish such services whenever the physician believes that this may benefit his or her patient. Physicians may also ethically teach in recognized schools of chiropractic. (V, VI)"[8]
British Medical Association[]
The British Medical Association notes that "There is also no problem with GPs [doctors] referring patients to practitioners in osteopathy and chiropractic who are registered with the relevant statutory regulatory bodies, as a similar means of redress is available to the patient."[43]
Safety[]
- See also: Spinal adjustment
The World Health Organization states that when "employed skilfully and appropriately, chiropractic care is safe and effective for the prevention and management of a number of health problems."[44] The International Chiropractic Association (ICA) suggests that chiropractic is one of the safest health professions and chiropractors have some of the lowest malpractice insurance premiums in the health care industry.[45] As with all interventions, there are risks associated with spinal manipulation. According to Harrison's, these include vertebrobasilar accidents (VBA), strokes, spinal disc herniation, vertebral fracture, and cauda equina syndrome. A 1996 Danish chiropractic study confirmed the risk of stroke to be low, and determined that the greatest risk is with manipulation of the first two vertebrae of the cervical spine, particularly passive rotation of the neck, known as the "master cervical" or "rotary break."[46] Estimates of serious complications range from 1 in 400,000 manipulations to 0 in 5 million manipulations. In comparison, there is a 3-4% rate of complications for cervical spine surgery, and 4,000-10,000 deaths per million neck surgeries. [47][48]
Practice styles and schools of thought[]
Contemporary chiropractic can be divided into several approaches to patient care: all are based on non-invasive, non-medication approaches, with many based on the use of manipulation as a treatment for mechanical musculoskeletal dysfunction of the spine and extremities. Most chiropractors advertise themselves as primary care doctors, and consider themselves part of "alternative health care", but there can be large differences between practitioners.[49] The differences between straights and mixers are reflected in multiple national practice associations, but most chiropractors are not members of any national organization.
- Traditional Straight chiropractors are the oldest movement. They adhere to the philosophical principles set forth by DD and BJ Palmer; that vertebral subluxation leads to interference of the human nervous system and is a primary underlying risk factor for almost any disease. Straights adhere to the chiropractic diagnosis of subluxations, and view the medical diagnosis of patient complaints (which they consider to be the "secondary effects" of subluxations) to be unnecessary for treatment. Instead, patients are typically screened for "red flags" of serious disease, and treated based on a practitioner's preferred chiropractic technique. This stance against medical diagnosing has been a source of contention between mixers and straights, because accreditation standards mandate that differential diagnosis be taught in all chiropractic programs so that patient care is safe and relevant to their complaints. Additionally, several state chiropractic licensing boards mandate that patient complaints be diagnosed before receiving care. The most popular national association for traditional straights is the International Chiropractors Association (ICA).
- Mixer chiropractors are an early offshoot of the straight movement. This branch originated from naturopathic, osteopathic, medical, and even chiropractic doctors who attended the Palmer College of Chiropractic and then re-organized the treatment system to include more diagnostic and treatment approaches. They eventually split from the traditional straight group and formed various other chiropractic schools including the National College of Chiropractic. Their treatments may include naturopathic remedies, physical therapy devices, or other CAM methods. While still subluxation based, mixers also treat problems associated with both the spine and extremities, including musculoskeletal issues such as pain and decreased range of motion. Mixers describe vertebral subluxations as a form of joint dysfunction or osteoarthritis. Diagnosis is made after ruling out other known disorders and noting general signs of mechanical dysfunction in the spine. They tend to be members of the American Academy of Chiropractic Physicians and or the American Chiropractic Association (ACA), and all the major groups in Europe are also in membership of the European Chiropractors Union.[50]
- Objective Straight chiropractors [51] are a recent off-shoot of the traditional straights and are a minority. This group is differentiated from traditional straights mainly by the claims made. While traditional straights claimed that chiropractic adjustments are a plausible treatment for a wide range of diseases, objective straights only focus on the correction of chiropractic vertebral subluxations. Like traditional straights, objective straights typically do not diagnose patient complaints. Their guiding principles are summed up as: "We do not want to diagnose and treat diseases, even diseases of the spine." and "We do not want chiropractic to be practiced as an alternative to medicine."[52] They also don't refer to other professionals, but do encourage their patients "to see a medical physician if they indicate that they want to be treated for the symptoms they are experiencing or if they would like a medical diagnosis to determine the cause of their symptoms".[53] Most objective straights limit treatment to spinal adjustments; they tend to be members of the Federation of Straight Chiropractors and Organizations (FSCO) and the World Chiropractic Alliance (WCA).
- Reform chiropractors are a minority group who advocate the use of palpation and manipulation to identify and treat osteoarthritis, painful joints, and other musculoskeletal problems. They do not subscribe to the Palmer philosophy of Innate Intelligence and vertebral subluxations, and tend not to use alternative medicine methods.
Education, licensing, and regulation[]
See main articles:
- Chiropractic education
- Chiropractic schools
- Council on Chiropractic Education
- Federation of Chiropractic Licensing Boards
- Chiropractors Locator (United States)
Today, there are 17 accredited chiropractic colleges in the USA and two in Canada, and an estimated 70,000 chiropractors in the USA, 5000 in Canada, 2500 in Australia, 1300 in the UK, and smaller numbers in about 50 other countries. In the USA and Canada, licensed individuals who practice chiropractic are commonly referred to as chiropractors, doctors of chiropractic (DC), or chiropractic physicians.
References[]
- ↑ Council on Chiropractic Education pdf see page 15
- ↑ Association of Chiropractic Colleges, Chiropractic Paradigm
- ↑ Federation of Chiropractic Licensing Boards, Questions and Answers about Professional Regulation and the Chiropractic Profession, Where are chiropractors regulated?, January 9, 2006.available online
- ↑ Michel Tetrault, DC, Country Chiropractic Support, Chiropractic Diplomatic Corps. available online
- ↑ Homola S, "Chiropractic, Bonesetting, and Cultism",Chiropractic, Bonesetting, and Cultism (entire book on-line)
- ↑ The Council on Chiropractic Education (2006), Standards for Doctor of Chiropractic Programs and Requirements for Institutional Status available online
- ↑ McDonald W (2003) How Chiropractors Think and Practice: The Survey of North American Chiropractors. Institute for Social Research, Ohio Northern University
- ↑ 8.0 8.1 McCrory DC, et al. Evidence Report: Behavioral and Physical Treatments for Tension-type and Cervicogenic Headache. Duke University Evidence-Based Practice Center, Durham, North Carolina, January 2001 available online (PDF format) Cite error: Invalid
<ref>tag; name "Duke" defined multiple times with different content - ↑ Ernst E (2006) A systematic review of systematic reviews of spinal manipulation J R Soc Med 99:192-6 Available on-line
- ↑ Balon J. (1998) A Comparison of Active and Simulated Chiropractic Manipulation as Adjunctive Treatment for Childhood Asthma. New Eng J Med 339:1013-20 available online
- ↑ Cite error: Invalid
<ref>tag; no text was provided for refs namedSciArtPhi - ↑ Cite error: Invalid
<ref>tag; no text was provided for refs namedForgotten Theories - ↑ 13.0 13.1 AHCPR Chapter II Chiropractic Belief Systems
- ↑ Morgan L (1998) Innate intelligence: its origins and problems J Can Chir Ass 42:35-41 available online
- ↑ Gatterman MI. Foundations of the Chiropractic Subluxation. Baltimore: Williams and Wilkins, 1988:6. referenced in
- ↑ Rosner A (2006) Occam's razor and subluxation: a close shave, Dynamic Chiropractic Aug 2006
- ↑ Nelson CF, Lawrence DJ, Triano JJ, Bronfort G, Perle SM, Metz RD, Hegetschweiler K, La Brot T. Chiropractic as spine care: a model for the profession. Chiropr Osteopat. 2005;13:9. doi: 10.1186/1746-1340-13-9. avaliable online
- ↑ Black D (1990)Inner Wisdom: The Challenge of Contextual Healing. Springville, UT: Tapestry Press
- ↑ More Than One-Third of U.S. Adults Use Complementary and Alternative Medicine, According to New Government Survey (Press Release), May 27 2004, available online
- ↑ Complementary and Alternative Medicine Use Among Adults: United States, 2002 (Report), May 27 2004, available online (PDF format)
- ↑ Burton, Bernard. "Chiropractic Management of Low Back Pain" Cleveland Clinic: Spinal Care 2000 Symposium. March 30, 2000.
- ↑ Bureau of Labor Statistics, Occupational Outlook Handbook
- ↑ Keating J. (1999), Tom Moore Defender of Chiropractic Part 1, Dynamic Chiropractic
- ↑ Phillips R (1998), Education and the Chiropractic Profession, Dynamic Chiropractic
- ↑ 25.0 25.1 Keating J Faulty Logic & Non-skeptical Arguments in Chiropractic
- ↑ Robbins J (1996),Medical monopoly: the game nobody wins - excerpt from 'Reclaiming Our Health: Exploding the Medical Myth and Embracing the Source of True Healing', Vegetarian Times available online
- ↑ 27.0 27.1 Wilk vs American Medical Association Summary
- ↑ Chirofind.com Chiropractic Research
- ↑ Biggs L (2002) Measuring philosophy: a philosophy index'' JCCA
- ↑ French S, Green S. The Cochrane Collaboration: is it relevant for doctors of chiropractic?. J Manip Physiol Ther 28: 641-2. PMID 16326231.
- ↑ Assendelft WJJ et al. (1996). The effectiveness of chiropractic for treatment of low back pain: an update and attempt at statistical pooling. J Manip Physiol Ther 19: 499-507. PMID 16326231.
- ↑ Meade et al. (1995). The effectiveness of chiropractic for treatment of low back pain: an update and attempt at statistical pooling. Brit Med J. PMID 16326231.
- ↑ Shekelle PM (1993) RAND misquoted. ACA J Chir 30:59–63
- ↑ Verhoef MJ, Costa Papadopoulos C. Survey of Canadian chiropractors’involvement in the treatment of patients under the age of 18. [1]
- ↑ Wiberg JMM et al. (1999) The short-term effect of spinal manipulation in the treatment of infantile colic: A randomized controlled clinical trial with a blinded observer. J Manip Physiol Ther 22:517-22[2]
- ↑ Olafsdottir E et al. (2001) Randomised controlled trial of infantile colic treated with chiropractic spinal manipulation. Arch Dis Child 84:138-141. [3]
- ↑ Keating J et al. (1998). A descriptive analysis of the Journal of Manipulative and Physiological Therapeutics, 1989-1996. J Manip Physiol Ther 21: 539-52. PMID 9798183.
- ↑ Manga P, Angus D. (1998) Enhanced Chiropractic Coverage Under OHIP as a Means of Reducing Health Care Costs, Attaining Better Health Outcomes and Achieving Equitable Access to Health Services. Retrieved 08 29 2006, from OCA
- ↑ Wolk S. (1988) An analysis of Florida workers' compensation medical claims for back-related injuries. J Amer Chir Ass 27:50-59
- ↑ Nyiendo J. (1991) Disability low back Oregon workers' compensation claims. Part II: Time loss. J Manip Physiol Ther 14:231-239
- ↑ Johnson M. (1989) A comparison of chiropractic, medical and osteopathic care for work-related sprains/strains. J Manip Physiol Ther 12:335-344
- ↑ Cherkin CD, MacCornack FA, Berg AO (1988) Managing low back pain. A comparison of the beliefs and behaviours of family physicians and chiropractors.West J Med 149:475–480
- ↑ British Medical Association, Referrals to complementary therapists
- ↑ WHO guidelines on basic training and safety in chiropractic, World Health Organization, Geneva, 2005. ISBN 92-4-159371-7. available online
- ↑ ICA website
- ↑ Klougart N, Leboeuf-Yde C, Rasmussen L. Safety in chiropractic practice, Part I; The occurrence of cerebrovascular accidents after manipulation to the neck in Denmark from 1978-1988.. J Manip Physiol Ther 19: 371-7. PMID 8864967.
- ↑ Coulter ID, Hurwitz EL, Adams AH, et al. (1996) The appropriateness of manipulation and mobilization of the cervical spine 'Santa Monica, CA, Rand Corp: xiv [RAND MR-781-CCR]. Current link
- ↑ Lauretti W "What are the risk of chiropractic neck treatments?" retrieved online 08 028 2006 from www.chiro.org
- ↑ James W. Healey, DC (1990) [http://www.chiroweb.com/archives/08/21/13.html It's Where You Put the Period. Dynamic Chiropractic October 10, 1990, Volume 08, Issue 21
- ↑ Souza T (2005) Differential Diagnosis and Management for the Chiropractor, Third Edition : Protocols and Algorithms Jones and Bartlett Publishers Inc. 3rd edition
- ↑ Position Paper One - What is Objective Straight Chiropractic?
- ↑ F.A.C.E. three guiding principles
- ↑ Position Paper Five - Referral
See also[]
- Applied kinesiology
- Joint manipulation
- Manipulative therapy
- Naprapathy
- Osteopathy
- Physical therapy
- Reflexology
External links[]
Professional organizations[]
- Academy of Upper Cervical Chiropractic Organizations (AUCCO)
- American Chiropractic Association (ACA)
- Association of Chiropractic Colleges (ACC)
- British Chiropractic Association (BCA)
- Canadian Chiropractic Association (CCA)
- Chiropractic Association of South Africa (CASA)
- Chiropractic Doctors' Association of Hong Kong (CDAHK)
- Christian Chiropractors Association (CCA)
- Council on Chiropractic Education - USA (CCE-USA)
- European Chiropractors' Union (ECU)
- Federation of Chiropractic Licensing Boards (FCLB) - Article here: Federation of Chiropractic Licensing Boards
- Federation of Straight Chiropractors and Organizations (FSCO)
- Foundation for the Advancement of Chiropractic Education (F.A.C.E.)
- Foundation for Chiropractic Education and Research (FCER)
- Hong Kong Chiropractors' Association (HKCA)
- International Chiropractic Pediatric Association (ICPA)
- International Chiropractors Association (ICA)
- Japanese Association of Chiropractors (JAC)
- McTimoney Chiropractic Association (MCA)
- National Association for Chiropractic Medicine (NACM)
- National Board of Chiropractic Examiners (NBCE)
- National Upper Cervical Chiropractic Association (NUCCA)
- National Upper Cervical Chiropractic Research Association (NUCCRA)
- United Chiropractic Association (UCA)
- World Chiropractic Alliance (WCA)
- World Federation of Chiropractic (WFC)
Chiropractic schools[]
- Main article: Chiropractic schools
Other resources[]
- The Chiropractic Resource Organization
- Chiropractic History Archive - Joseph C. Keating Jr, PhD
- The Chiropractic Profession and Its Research and Education Programs
- Chiropractic in the United States: Training, Practice, and Research (1997) - Cherkin, Daniel C.; Mootz, Robert D.
- Chiropractic treatments for back pain - Steven G. Yeomans, DC. A Spine-health.com feature (use menu points on left side)
- Dynamic Chiropractic Online - ChiroWeb, Chiropractic news source
- National Directory of Chiropractic - Listing of Chiropractors and information on education and the profession.
- National Center for Complementary and Alternative Medicine - National Institute of Health - Manipulative and Body-Based Practices
- The Future of Chiropractic Revisited: 2005 to 2015
- Olympic Games Inspire Optimal Athletic Care
Internal criticism[]
- Samuel Homola DC, a notable and outspoken dissident within the profession, expresses his opinion that evidence-based chiropractic is the only way forward.
- Chiropractic, Bonesetting, and Cultism - Samuel Homola (entire book on-line).
- This book, published in 1964, contains trenchant criticism of the profession, and the following year Homola's application to renew his membership of the ACA was rejected. In 1991, David J. Redding, chairman of the ACA board of governors, welcomed Homola back to membership of the ACA, and in 1994, 30 years after its publication, the book was reviewed for the first time by a chiropractic journal. [9]
- JC Smith, a chiropractor in private practice, writes in 1999 that ethical issues are "in dire need of debate" because of "years of intense medical misinformation/slander" and because of well publicised examples of tacky advertising, outlandish claims, sensationalism and insurance fraud.
- Joseph C. Keating, Jr, PhD, professor at the Los Angeles College of Chiropractic and notable historian of chiropractic, warns of pseudoscientific notions that still persist in the mindsets of some chiropractors
- Dr Keating critically distinguishes between sound and unsound arguments in support of chiropractic
- Christopher Kent, DC president of the Council on Chiropractic Practice, advises his colleagues of the importance of high standards of evidence, noting that in the past chiropractors were too ready to accept anecdotal evidence
- Open Letter to the Profession (See Chiroweb for commentary.)
- A 1992 letter from ACA attorney, George P. McAndrews, warns the chiropractic profession that advertising of scare tactic subluxation philosophy damages the newly won respect within the AMA.
- A 1991 editorial from chiropractic trade magazine, Dynamic Chiropractic, where Joseph C. Keating Jr discusses his concerns for advertising products before they are scientifically evaluated.
- A 2000 commentary by Ronald Carter, DC, MA, Past President, Canadian Chiropractic Association in the Journal of the Canadian Chiropractic Association discussing his opinion that the subluxation story regardless of how it is packaged is not the answer. He suggests it is now time for the silent majority to make their voices heard and come together to present a rational and defensible model of chiropractic so that is not just included in the health care system, but an essential member of the health care team.
External criticism[]
- Keeping Your Spine In Line, Adjusting the Joints, and Video - Alan Alda, PBS, Scientific American Frontiers, Web Feature (combines internal and external criticism)
- Chirobase: Skeptical guide to chiropractic history, theories, and current practices - Stephen Barrett, MD, and Samuel Homola, DC (combines internal and external criticism)
- Chiropractic: Flagship of the Alternative Medicine Fleet, Part One and Part Two - by Steven Novella MD, and President of the New England Skeptical Society
- Chiropractor Adelaide: For additional information on Chiropractor
Abbreviations[]
- AMA, The American Medical Association
- BMJ, The British Medical Journal
- DC, Doctor of Chiropractic
- FDA, Food and Drug Administration
- JMPT, The Journal of Manipulative and Physiological Therapeutics
de:Chiropraktik nl:Chiropractie fi:Kiropraktiikka pt:Quiropraxia sv:Kiropraktik ur:معالجہ بالید
| This page uses Creative Commons Licensed content from Wikipedia (view authors). |