Assessment |
Biopsychology |
Comparative |
Cognitive |
Developmental |
Language |
Individual differences |
Personality |
Philosophy |
Social |
Methods |
Statistics |
Clinical |
Educational |
Industrial |
Professional items |
World psychology |
Clinical: Approaches · Group therapy · Techniques · Types of problem · Areas of specialism · Taxonomies · Therapeutic issues · Modes of delivery · Model translation project · Personal experiences ·
| ICD-10 | H903-H905 | |
|---|---|---|
| ICD-9 | 389.1 | |
| OMIM | [1] | |
| DiseasesDB | 2874 | |
| MedlinePlus | [2] | |
| eMedicine | / | |
| MeSH | {{{MeshNumber}}} | |
- Main article: Hearing disorders
| Sensorineural hearing loss | |
|---|---|
| Classification and external resources | |
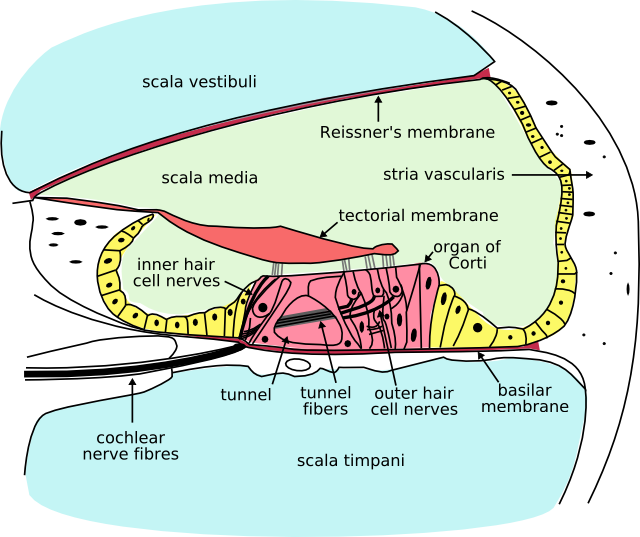 Cross section of the cochlea. | |
| ICD-10 | H903-H905 |
| ICD-9 | 389.1 |
| DiseasesDB | 2874 |
| MeSH | D006319 |
Sensorineural hearing loss (SNHL) is a type of hearing loss in which the root cause lies in the vestibulocochlear nerve (Cranial nerve VIII), the inner ear, or central processing centers of the brain.
The Weber test, in which a tuning fork is touched to the midline of the forehead, localizes to the normal ear in people with this condition. The Rinne test, which tests air conduction vs. bone conduction is positive (normal), though both bone and air conduction are reduced equally.
Sensorineural hearing loss can be mild, moderate, or severe, including total deafness.
The great majority of human sensorineural hearing loss is caused by abnormalities in the hair cells of the organ of Corti in the cochlea. There are also very unusual sensorineural hearing impairments that involve the eighth cranial nerve (the vestibulocochlear nerve) or the auditory portions of the brain. In the rarest of these sorts of hearing loss, only the auditory centers of the brain are affected. In this situation, central hearing loss, sounds may be heard at normal thresholds, but the quality of the sound perceived is so poor that speech can not be understood.
Most sensory hearing loss is due to poor hair cell function. The hair cells may be abnormal at birth, or damaged during the lifetime of an individual. There are both external causes of damage, like noise trauma and infection, and intrinsic abnormalities, like deafness genes.
Sensory hearing loss that results from abnormalities of the central auditory system in the brain is called central hearing impairment. Since the auditory pathways cross back and forth on both sides of the brain, deafness from a central cause is unusual.
This type of hearing loss can also be caused by prolonged exposure to very loud noise, for example, being in a loud workplace without hearing protection, or having headphones set to high volumes for a long period.
Differential diagnosis[]
Table 1. A table comparing sensorineural to conductive hearing loss
| Criteria | Sensorineural hearing loss | Conductive hearing loss |
| Anatomical Site | Inner ear, cranial nerve VIII, or central processing centers | Middle ear (ossicular chain), tympanic membrane, or external ear |
| Weber Test | Sound localizes to normal ear | Sound localizes to affected ear (ear with conductive loss) |
| Rinne Test | Positive Rinne; Air conduction > Bone conduction (both air and bone conduction are decreased equally, but the difference between them is unchanged). | Negative Rinne; Bone Conduction > Air Conduction (Bone/Air Gap) |
Sensorineural hearing loss may be congenital or acquired.
Congenital[]
- Lack of development (aplasia) of the cochlea
- Chromosomal syndromes (rare)
- Congenital cholesteatoma - squamous epithelium is normally present on either side of the tympanic membrane. Externally, within the external auditory meatus or ear canal and internally within the middle ear. Within the middle ear the simple epithelium gradually transitions into ciliated pseudostratified epithelium lining the Eustachian tube now known as the pharyngotympanic tube becoming continuous with the respiratory epithelium in the pharynx. The squamous epithelium hyperplasia within the middle ear behaves like an invasive tumour and destroys middle ear structures if not removed.
- Delayed familial progressive
Acquired[]
- Inflammatory
- Suppurative labyrinthitis
- Meningitis
- Mumps
- Measles
- Viral
- Syphilis
- Ototoxic drugs
- Aminoglycosides (most common cause; e.g., tobramycin)
- Loop diuretics (e.g., furosemide)
- Antimetabolites (e.g., methotrexate)
- Salicylates (e.g., aspirin)
- Physical trauma - either due to a fracture of the temporal bone affecting the cochlea and middle ear, or a shearing injury affecting cranial nerve VIII.
- Noise-induced - prolonged exposure to loud noises (>90 dB) causes hearing loss which begins at 4000 Hz (high frequency). The normal hearing range is from 20 Hz to 20,000 Hz.
- Presbycusis - age-related hearing loss that occurs in the high frequency range (4000 Hz to 8000 Hz).
- Sudden hearing loss
- Idiopathic (ISSHL: idiopathic sudden sensoneurinal hearing loss), H91.2
- Vascular ischemia of the inner ear or CN 8
- Perilymph fistula, usually due to a rupture of the round or oval windows and the leakage of perilymph. The patient will most likely also experience vertigo or imbalance. A history of an event that increased intracranial pressure or caused trauma is usually present).
- Autoimmune - can be due to an IgE or IgG allergy (e.g. food)
- Autoimmune - a prompt injection of steroids into ear is necessary.[citation needed]
- Cerebellopontine angle tumour (junction of the pons and cerebellum) (the cerebellopontine angle is the exit site of both the facial nerve(CN7) and the vestibulocochlear nerve(CN8). Patients with these tumors often have signs and symptoms corresponding to compression of both nerves)
- Acoustic neuroma (vestibular schwannoma) - this is a schwannoma (benign neoplasm of Schwann cells)
- Meningioma - benign tumour of the pia and arachnoid maters
- Ménière's disease - causes sensorineural hearing loss in the low frequency range (125 Hz to 1000 Hz). Ménière's disease is characterized by sudden attacks of vertigo, lasting minutes to hours preceded by tinnitus, aural fullness, and fluctuating hearing loss.
Long term exposure to environmental noise[]
Populations living near airports or freeways are exposed to levels of noise typically in the 65 to 75 dbA range. If lifestyles include significant outdoor or open window conditions, these exposures over time can degrade hearing. The U.S. EPA and various states have set noise standards to protect people from these adverse health risks. The EPA has identified the level of 70 db(A) for 24 hour exposure as the level necessary to protect the public from hearing loss (EPA, 1974).
- Noise-induced hearing loss (NIHL) typically is centered at 4000 Hz.
- The louder the noise is, the shorter the safe amount of exposure is. Normally, the safe amount of exposure is reduced by a factor 2 for every additional 3 dB. For example, the safe daily exposure amount at 85 dB is 8 hours, while the safe exposure at 91 dB(A) is only 2 hours (National Institute for Occupational Safety and Health, 1998). Sometimes, a factor 2 per 5 dB is used.
- Personal audio electronics, such as iPods (iPods often reaching 115 decibels or higher), can produce powerful enough sound to cause significant NIHL, given that lesser intensities of even 70 dB can also cause hearing loss.[1]
Genetic[]
Hearing loss can be inherited. Both dominant and recessive genes exist which can cause mild to profound impairment. If a family has a dominant gene for deafness, it will persist across generations because it will manifest itself in the offspring even if it is inherited from only one parent. If a family had genetic hearing impairment caused by a recessive gene, it will not always be apparent, as it will have to be passed onto offspring from both parents. Dominant and recessive hearing impairment can be syndromic or nonsyndromic. Recent gene mapping has identified dozens of nonsyndromic dominant (DFNA#) and recessive (DFNB#) forms of deafness.
- The most common type of congenital hearing impairment in developed countries is DFNB1, also known as Connexin 26 deafness or GJB2-related deafness.
- The most common dominant syndromic forms of hearing impairment include Stickler syndrome and Waardenburg syndrome.
- The most common recessive syndromic forms of hearing impairment are Pendred syndrome, large vestibular aqueduct syndrome and Usher syndrome.
- MT-TL1 mutations cause hearing loss, along with diabetes and other symptoms.
Disease or illness[]
- Measles may result in auditory nerve damage
- Meningitis may damage the auditory nerve or the cochlea
- Autoimmune disease has only recently been recognized as a potential cause for cochlear damage. Although probably rare, it is possible for autoimmune processes to target the cochlea specifically, without symptoms affecting other organs. Wegener's granulomatosis, an autoimmune condition, may precipitate hearing loss.
- Autoinflammatory disease, such as Muckle-Wells Syndrome, can lead to hearing loss.
- Mumps (epidemic parotitis) may result in profound sensorineural hearing loss (90 dB or more), unilaterally (one ear) or bilaterally (both ears).
- Presbycusis is deafness due to loss of perception to high tones, mainly in the elderly. It is considered by some to be a degenerative process, although there has never been a proven link to aging. (See impact of environmental noise exposure above.)
- Adenoids that do not disappear by adolescence may continue to grow and may obstruct the Eustachian tube, causing conductive hearing impairment and nasal infections that can spread to the middle ear.
- AIDS and ARC patients frequently experience auditory system anomalies.[2]
- HIV (and subsequent opportunistic infections) may directly affect the cochlea and central auditory system.[2]
- Chlamydia may cause hearing loss in newborns to whom the disease has been passed at birth.[2]
- Fetal alcohol syndrome is reported to cause hearing loss in up to 64% of infants born to alcoholic mothers, from the ototoxic effect on the developing fetus, plus malnutrition during pregnancy from the excess alcohol intake.[2]
- Premature birth results in sensorineural hearing loss approximately 5% of the time.[2]
- Syphilis is commonly transmitted from pregnant women to their fetuses, and about a third of the infected children will eventually become deaf.[2]
- Otosclerosis is a hardening of the stapes (or stirrup) in the middle ear, and causes conductive hearing loss.
Medications[]
- See also Ototoxicity
Some medications cause irreversible damage to the ear, and are limited in their use for this reason. The most important group is the aminoglycosides (main member gentamicin).
Various other medications may reversibly affect hearing. This includes some diuretics, sildenafil and NSAIDs, and macrolide antibiotics.
Extremely heavy hydrocodone (Vicodin) abuse is known to cause hearing impairment. There has been speculation radio talk show host Rush Limbaugh's hearing loss was at least in part caused by his admitted addiction to narcotic pain killers, in particular Vicodin and OxyContin. [needs citation]
Physical trauma[]
- There can be damage either to the ear itself or to the brain centers that process the aural information conveyed by the ears.
- People who sustain head injury are especially vulnerable to hearing loss or tinnitus, either temporary or permanent.
- Exposure to very loud noise (90 dB or more, such as jet engines at close range) can cause progressive hearing loss. Exposure to a single event of extremely loud noise (such as explosions) can also cause temporary or permanent hearing loss. A typical source of acoustic trauma is a too-loud music concert.[3]
Treatment[]
Previously, sensorineural hearing loss has been treated with hearing aids, which amplify sounds at preset frequencies to overcome a sensorineural hearing loss in that range; or cochlear implants, which stimulate the cochlear nerve directly.
Some research suggests idebenone alone or combined with vitamin E may delay the onset of hearing loss or perhaps reverse it.[4] Use of these agents for this purpose is considered experimental now.
Some audiologists and ENTs have reported if severe noise-induced hearing loss (exposures exceeding 140dB) is treated immediately (within 24 hours) with a course of steroids, it can often be almost completely reversed.[citation needed] This, however, is a new field without proven success.[5]
Researchers at the University of Michigan report that a combination of high doses of vitamins A, C, and E, and Magnesium, taken one hour before noise exposure and continued as a once-daily treatment for five days, was very effective at preventing permanent noise-induced hearing loss in animals[6]
References[]
- ↑ Sound Output Levels of the iPod and Other MP3 Players: Is There Potential Risk to Hearing?. URL accessed on 2007-11-20.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 Frequently Asked Questions: Etiologies and Causes of Deafness. URL accessed on 2006-12-02.
- ↑ Hearing Loss News and Articles: Sonic tonic
- ↑ Sergi, Bruno (2006). Neuroreport 17 (9): 857–861.
- ↑ Haynes, David S. (2009). The Laryngoscope 117 (1): 3–15.
- ↑ http://www.hearinglossweb.com/Medical/Causes/nihl/prtct/nutr.htm
External links[]
- A free online hearing test to measure your ears' high frequency response
- Hearing Loss Web
- Sensorineural Hearing Loss, Dr Peter Grant [dead link]
Diseases of the ear and mastoid process (H60-H99, 380-389) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outer ear |
Otitis externa ·Otomycosis | ||||||||||||||||||
| Middle ear and mastoid |
Otitis media · Mastoiditis (Bezold's abscess, Gradenigo's syndrome) · Tympanosclerosis Cholesteatoma · Perforated eardrum | ||||||||||||||||||
| Inner ear and central pathways |
| ||||||||||||||||||
| {| class="navbox collapsible nowraplinks" style="margin:auto; " | |||||||||||||||||||
| |||||||||||||||||||
|}
| This page uses Creative Commons Licensed content from Wikipedia (view authors). |